http://www.campaigntoendloneliness.org/wp-content/uploads/Loneliness-Measurement-Guidance1-1.pdf
bone = minerals = calcium + phosphates
Cells in bones that are making new bones & destroying old bones = laying down cement to make a road & cutting up and shaking up the old roads => needs to rebuild every once in a while
Same progenitor = osteoClasts/osteoBlasts
Bone resorption = osteoClasts
Low calcium = body will resorb bones to correct hypoglycemia
Need calcium in blood for muscle & heart & lots of things
Denosumab needs to make bones, & they are osteoclasts. So, they'll need to break bones. If you are already hypocalcemia, the body needs to break bones to build new bones & also need to break bones to provide more bones in the blood => need to correct for hypocalcemia
bone turnover = body still needs to find the balance btw bone resorption & bone clast.
Cells in bones that are making new bones & destroying old bones = laying down cement to make a road & cutting up and shaking up the old roads => needs to rebuild every once in a while
Same progenitor = osteoClasts/osteoBlasts
Bone resorption = osteoClasts
Low calcium = body will resorb bones to correct hypoglycemia
Need calcium in blood for muscle & heart & lots of things
Denosumab needs to make bones, & they are osteoclasts. So, they'll need to break bones. If you are already hypocalcemia, the body needs to break bones to build new bones & also need to break bones to provide more bones in the blood => need to correct for hypocalcemia
bone turnover = body still needs to find the balance btw bone resorption & bone clast.
PO (oral pills only): Amoxicillin/clavulanic acid (Augmentin)
IV: ampicillin/sulbactam (Unasyn)
IV: piperacillin/tazobactam (Zosyn) ==> the only one with pseudomonas as well
QID: ticarcillin/clavulanic acid (Timentin)
HA-PNA => MRSA, Pseudomonas
MRSA PNA => Vancomycin
MRSA Pseudomonas => Zosyn (pipercillin/tazobactam)
MRSA PNA => Vancomycin
MRSA Pseudomonas => Zosyn (pipercillin/tazobactam)
Disease => Bacteria => Side Effects => Route of administration
In statistics, the Pearson product-moment correlation coefficient (/ˈpɪərsᵻn/) (sometimes referred to as the PPMCC or PCC or Pearson's r) is a measure of the linear correlation between two variables X and Y, giving a value between +1 and −1 inclusive, where 1 is total positive correlation, 0 is no correlation, and −1 ...
Sometimes I ponder on the so-called 't'nh dda`n ba`'. Why is that being
petty so associated with women? I think about all the social suppression
on females in many male-dominated cultures: females not considered for
certain jobs, even in female dominated fields if she lets it known that
she may be pregnant, women earning less, etc. Why is that? I deem it's
because of the lack of resources that women have. The less resources you
have, the more violent and petty you are. Because
of the women's physique, they can't actually be overtly violent, they
turn out to be passive-aggressive and petty. In a few other minority
'exotic' tribal cultures in which women are dominated, they also exhibit
these so-called gender-assigned male traits: chasing for mates, etc. I
wonder if it's 'ti'nh dda`n ba`' should be reassigned as
lack-of-resources and vice versa.....
Testing with success series
followed by three to five options:Test strategies:
Cover the options, read the stem, and try to answer
Select the option that most closely matches your answer
Read the stem with each option
Treat each option as a true-false question, and choose the "most true"
Strategies for answering difficult questions:
not only a correct one, and not one which must be true all of the time, in all cases, and without exception
Source: http://www.studygs.net/tsttak3.htm
See also:
http://www.rcsdk12.org/cms/lib04/NY01001156/Centricity/Domain/4932/multiple-choice%20strategies.pdf
http://www2.isu.edu/success/strategies/handouts/docs/test_taking_and_money/Systematic%20Method%20of%20Answering%20Multiple%20Choice%20Questions.pdf
Multiple choice tests
Multiple choice questions usually include a phrase or stemfollowed by three to five options:Test strategies:
- Read the directions carefully
Know if each question has one or more correct option
Know if you are penalized for guessing
Know how much time is allowed (this governs your strategy) - Preview the test
Read through the test quickly and answer the easiest questions first
Mark those you think you know in some way that is appropriate - Read through the test a second time and answer more difficult
questions
You may pick up cues for answers from the first reading, or become more comfortable in the testing situation - If time allows, review both questions and answers
It is possible you mis-read questions the first time
Cover the options, read the stem, and try to answer
Select the option that most closely matches your answer
Read the stem with each option
Treat each option as a true-false question, and choose the "most true"
Strategies for answering difficult questions:
- Eliminate options you know to be incorrect
If allowed, mark words or alternatives in questions that eliminate the option - Give each option of a question the "true-false test:"
This may reduce your selection to the best answer - Question options that grammatically don't fit with the stem
- Question options that are totally unfamiliar to you
- Question options that contain negative or absolute words.
Try substituting a qualified term for the absolute one.
For example, frequently for always; or typical for every to see if you can eliminate an option - "All of the above:"
If you know two of three options seem correct, "all of the above" is a strong possibility - Number answers:
toss out the high and low and consider the middle range numbers - "Look alike options"
probably one is correct; choose the best but eliminate choices that mean basically the same thing, and thus cancel each other out - Double negatives:
Create the equivalent positive statement - Echo options:
If two options are opposite each other, chances are one of them is correct - Favor options that contain qualifiers
The result is longer, more inclusive items that better fill the role of the answer - If two alternatives seem correct,
compare them for differences,
then refer to the stem to find your best answer
- Always guess when there is no penalty
for guessing or you can eliminate options - Don't guess if you are penalized for guessing
and if you have no basis for your choice - Use hints from questions you know
to answer questions you do not. - Change your first answers
when you are sure of the correction, or other cues in the test cue you to change.
not only a correct one, and not one which must be true all of the time, in all cases, and without exception
Source: http://www.studygs.net/tsttak3.htm
See also:
http://www.rcsdk12.org/cms/lib04/NY01001156/Centricity/Domain/4932/multiple-choice%20strategies.pdf
http://www2.isu.edu/success/strategies/handouts/docs/test_taking_and_money/Systematic%20Method%20of%20Answering%20Multiple%20Choice%20Questions.pdf
A nurse practitioner student's diary & notes. I WANNA DO WELL. “You can't hope yourself to a better life, you must take yourself there. What you have to do is work with the raw material you have, namely you, and never let up. There is no way to succeed and have the lovely spoils - money, recognition, deep satisfaction in ur work - except to put in the hrs, do the drudgery. If you give, you get. If you work hard, the hard work rewards you." ~H.B.
Step III – Immunomodulators
Immune modifiers have a slower onset of action (typically, a 2- to 3-month lag) and, consequently, are not used for induction of remission. However, these agents have shown effectiveness for their steroid-sparing action in persons with refractory disease; they are also used as primary treatment for fistulas and maintenance of remission in patients intolerant of or not responsive to aminosalicylates.
The immunomodulators 6-mercaptopurine (6-MP) and azathioprine (AZA) are used in patients with inflammatory bowel disease (IBD) in whom remission is difficult to maintain with the aminosalicylates alone. Calcineurin inhibitors such as cyclosporin A (CSA) and tacrolimus, as well as methotrexate (MTX), are also immune-modifying agents[3] ; CSA is almost exclusively limited to acute severe colitis, whereas tacrolimus has been used in both perianal Crohn disease and ulcerative colitis.[3]
Data on MTX support the use of intramuscular MTX in Crohn disease, but such data are lacking in ulcerative colitis. The only trial of MTX in ulcerative colitis used a low-dose oral therapy[91] ; whether a higher-dose oral MTX or parenteral MTX (IM or SQ) may be effective in ulcerative colitis has not been studied. Several clinical trials showed that AZA continuation in patients with ulcerative colitis prevented relapse, as compared to those who discontinued the medication. However, other trials have shown trends but no statistically significant benefit of AZA in ulcerative colitis.[92]
source: http://patient.info/health/aminosalicylates
For example:
- If your condition affects the back passage (rectum) only, you may be prescribed an aminosalicylate suppository or enema.
- If your gut is affected higher up, you may be prescribed an aminosalicylate tablet:
- Mezavant®, Dipentum®, and Colazide® target the colon.
- Asacol®, Ipocol®, Mesren®, and Salofalk®, work a little higher in the gut in the last part of the small intestine (called the ileum).
- Pentasa® is designed to work along the entire length of the gut

Source: http://www.ccfa.org/assets/pdfs/aminosalicylates.pdf
Step I - Aminosalicylates
The 5 oral aminosalicylate preparations available for use in the United States are sulfasalazine (Azulfidine), mesalamine (Asacol, Asacol HD, Pentasa, Lialda, Apriso), balsalazide (Colazal), and olsalazine (Dipentum). Enema and suppository formulations are also available. All of these are derivatives of 5-aminosalicylic acid (5-ASA); the major differences are in the mechanism and site of delivery. Some of these agents also have unique adverse effects lacking in other agents of this class.
All of the aminosalicylates are useful for treating flares of IBD and for maintaining remission. None of the aminosalicylates has been proven to have greater efficacy than any of the others for the treatment of ulcerative colitis. As a class, these agents appear to be more effective in persons with ulcerative colitis than in persons with Crohn disease; in persons with mild Crohn disease, the primary utility is for colonic disease (as is the case with sulfasalazine[3] ; administer folic acid if sulfasalazine is used). Aminosalicylates have only a weak effect in preventing recurrence after surgery in patients with Crohn disease.[84]
For patients in remission from distal ulcerative colitis, oral or rectal 5-ASA can be used to manage this disease, as well as a combination regimen of oral and topical 5-ASA.[3] In treating rectal disease, rectal 5-ASA is preferred over rectal steroids.[3]A dose response has been described regarding the use of these agents for ulcerative colitis. For moderate disease, a dose of 4.8 g/day of mesalamine has been shown to be more efficacious than 2.4 g/day.[85]
Types and Administrative Methods There are a number of 5-ASA medications which differ based on primary medication type, medication coating, or route of administration (oral vs. rectal). The first 5-ASA widely used in IBD was sulfasalazine (Azulfidine®). Sulfasalazine is still used, however, some patients experience side effects due to the sulfa component (see below). Another form of 5-ASA is known as mesalamine, which does not contain a sulfa group. Approximately 90% of those with intolerance to sulfasalazine can tolerate mesalamine. There are several mesalamine-based oral 5-ASA agents including, Asacol®HD, Pentasa®, Lialda®, Apriso™, Delzicol™. These agents all use the same mesalamine, but differ in terms of the medication coating. Mesalamine must be coated or placed in special capsules to ensure drug delivery to the intestine or colon. The difference in coating affects where the medication is released in the intestine or colon and how frequently the medication needs to be taken (once, twice, or three times daily). Other forms of 5-ASA used include olsalazine (Dipentum®) or balsalazide (Colazal™), which are also effective therapies for ulcerative colitis. In many situations, rectal therapies using 5-ASA agents can dramatically improve control of IBD. Rectal administration permits delivery of high dose therapy (targeted exactly where it is needed) and avoids systemic (body wide) exposure. In many cases, rectal therapies are used in conjunction with oral therapies for additional symptom improvement:
• Suppositories (Canasa®) deliver mesalamine directly to the rectum. A high proportion of patients with proctitis (inflammation in the rectum) will respond to mesalamine suppositories. These are usually given in single or twice-daily doses and can provide substantial relief from the urgency and frequency of bowel movements. A suppository is inserted into the rectum and does not need to be passed or removed. A combination of rectal and oral therapies may be more effective than pills alone.
• Enema formulations (Rowasa®) allow mesalamine to be applied directly to the left colon, reaching higher than the suppository alone. Up to 80 percent of patients with left-sided colon inflammation benefit from using this therapy once a day. Enemas are liquid and should remain in the colon for at least 20-40 minutes.
Source: http://emedicine.medscape.com/article/179037-treatment#d11
Overview of Stepwise Therapy
A stepwise approach (now generally referred to as the step-up approach), such as outlined in the following sections, may be taken in mild to very moderate inflammatory bowel disease (IBD).
The first step in medication therapy for IBD is usually aminosalicylates. There are several different aminosalicylates, but none have been consistently demonstrated to be superior to the others for all patients. These agents appear to have greater efficacy for the treatment of ulcerative colitis than for Crohn disease, for which efficacy data are limited. For Crohn disease, metronidazole or ciprofloxacin is occasionally used, particularly for perianal disease or an inflammatory mass.
If the patient's condition fails to respond to an adequate dose of aminosalicylates, the second step is often corticosteroids, which tend to provide rapid relief of symptoms and a significant decrease in inflammation.[82] The most common range for moderate flares of IBD is oral prednisone at 10-40 mg/day; for more severe flares, the higher end of the range is used (occasionally doses up to 60 mg/day are required). Once a clinical response is seen, the dose is tapered. Most patients who use oral corticosteroids can tolerate a relatively rapid taper after a response is achieved; occasionally, a very prolonged steroid taper is necessary to prevent relapse in patients who have had prolonged exposure to steroids in the past. Inability to taper down the steroids without recurrence of symptoms should trigger discussion regarding the use of alternative drugs (immunomodulators or anti-TNF therapy).
The immune-modifying agents are step III drugs and are used if corticosteroids fail or are required for prolonged periods. Anti-TNF monoclonal antibody therapies are also step III drugs that are effective in both Crohn disease and ulcerative colitis; some studies have demonstrated that they have a greater efficacy than azathioprine.
Drugs from different therapeutic classes may be used additively. In some patients with high-risk disease, a step-down approach with early introduction of stronger agents such as the anti-TNF agents has been advocated to prevent complications and improve patient outcomes. There are many situations, especially in patients with more severe disease, where the step-down approach is clearly in the patient’s best interest.
In general, one major goal is to wean the patient off steroids as soon as possible to prevent long-term adverse effects from these agents. Ardizzone et al suggest that a lack of mucosal healing after corticosteroid therapy is the only factor associated with negative outcomes at 5 years
Source: http://emedicine.medscape.com/article/179037-treatment#d10
Supportive care
IBD flares in patients with mild to moderate disease are usually managed in an outpatient setting. However, an important and sometimes overlooked concern in the management of IBD is the dosing and duration of use of corticosteroid therapy. For a flare of moderate severity, a dose of prednisone of 20-40 mg/day or equivalent is often sufficient to treat the flares. Once symptoms are controlled, a dedicated tapering progression of the steroid follows.
Patients are candidates for immunomodulators (azathioprine, 6-mercaptopurine, methotrexate) or anti-TNF agents (infliximab, adalimumab, certolizumab pegol) and biologic agents if flares are frequent (>1-2 times), if the duration of steroid use is prolonged (more than a few weeks per year), if reduction of the steroid dose causes recurrence of symptoms (steroid dependent), or if steroids do not appear to be working (steroid refractory).
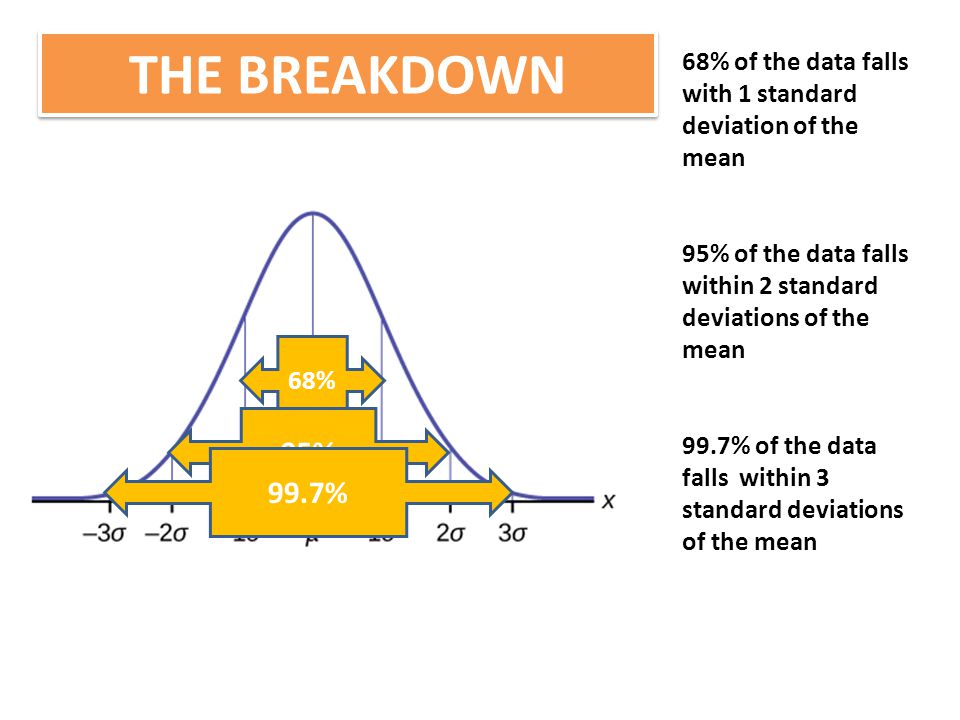
A health maintenance issue of particular importance to patients with IBD is a reduction in bone density because of decreased calcium absorption (due to the underlying disease process) or corticosteroid use. Osteoporosis is a very serious complication, involving 40% of patients with IBD, and increases the risk for fractures. All patients who have been using steroids for longer than 3 months, as well as postmenopausal women, should undergo testing with bone-density studies; treatment with bisphosphonates and calcium supplements can be initiated in patients with significantly low bone density.
Symptomatic therapy
In addition to treatment of the underlying inflammation, patients with inflammatory bowel disease (IBD) may require symptomatic therapy, particularly when their symptoms are not related to active inflammation. Treatment with antidiarrheal agents such as loperamine or diphenoxylate/atropine should generally be avoided in patients with active inflammation, as these drugs can precipitate toxic megacolon in individuals with significant colonic inflammation. Similarly, other agents that may have anticholinergic effects should be avoided, although antispasmodic medications may sometimes be useful for symptomatic relief. In patients with Crohn disease who have significant ileal disease or who have had an ileal resection, diarrhea may sometimes be due to bile salt malabsorption. In such patients, treatment with bile-binding resins, such as cholestyramine, may be helpful in managing the diarrhea.
source: http://www.mayoclinic.org/diseases-conditions/intestinal-obstruction/home/ovc-20168459
Intestinal obstruction is a blockage that keeps food or liquid from passing through your small intestine or large intestine (colon). Causes of intestinal obstruction may include fibrous bands of tissue (adhesions) in the abdomen that form after surgery, an inflamed intestine (Crohn's disease), infected pouches in your intestine (diverticulitis), hernias and colon cancer.
Without treatment, the blocked parts of the intestine can die, leading to serious problems. However, with prompt medical care, intestinal obstruction often can be successfully treated.
Causes
The most common causes of intestinal obstruction in adults are:
- Intestinal adhesions — bands of fibrous tissue in the abdominal cavity that can form after abdominal or pelvic surgery
- Colon cancer
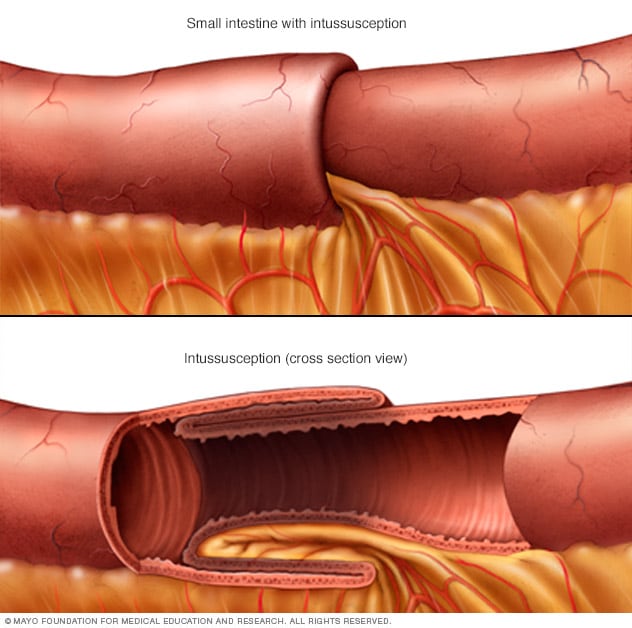
In children, the most common cause of intestinal obstruction is telescoping of the intestine (intussusception).
Other possible causes of intestinal obstruction include:
- Hernias — portions of intestine that protrude into another part of your body
- Inflammatory bowel diseases, such as Crohn's disease
- Diverticulitis — a condition in which small, bulging pouches (diverticula) in the digestive tract become inflamed or infected
- Twisting of the colon (volvulus)
- Impacted feces
Complications
Untreated, intestinal obstruction can cause serious, life-threatening complications, including:
- Tissue death. Intestinal obstruction can cut off the blood supply to part of your intestine. Lack of blood causes the intestinal wall to die. Tissue death can result in a tear (perforation) in the intestinal wall, which can lead to infection.
- Infection. Peritonitis is the medical term for infection in the abdominal cavity. It's a life-threatening condition that requires immediate medical and often surgical attention.
Treating intussusception
A barium or air enema is used both as a diagnostic procedure and a treatment for children with intussusception. If an enema works, further treatment is usually not necessary.
Treatment for partial obstruction
If you have an obstruction in which some food and fluid can still get through (partial obstruction), you may not need further treatment after you've been stabilized. Your doctor may recommend a special low-fiber diet that is easier for your partially blocked intestine to process. If the obstruction does not clear on its own, you may need surgery to relieve the obstruction.
Treatment for complete obstruction
If nothing is able to pass through your intestine, you'll usually need surgery to relieve the blockage. The procedure you have will depend on what's causing the obstruction and which part of your intestine is affected. Surgery typically involves removing the obstruction, as well as any section of your intestine that has died or is damaged.
Alternatively, your doctor may recommend treating the obstruction with a self-expanding metal stent. The wire mesh tube is inserted into your colon via an endoscope passed through your mouth or colon. It forces open the colon so that the obstruction can clear.
Stents are generally used to treat people with colon cancer or to provide temporary relief in people for whom emergency surgery is too risky. You may still need surgery, once your condition is stable.
Treatment for pseudo-obstruction
If your doctor determines that your signs and symptoms are caused by pseudo-obstruction (paralytic ileus), he or she may monitor your condition for a day or two in the hospital, and treat the cause if it's known. Paralytic ileus can get better on its own. In the meantime, you'll likely be given food through a nasal tube or an IV to prevent malnutrition.
If paralytic ileus doesn't improve on its own, your doctor may prescribe medication that causes muscle contractions, which can help move food and fluids through your intestines. If paralytic ileus is caused by an illness or medication, the doctor will treat the underlying illness or stop the medication. Rarely, surgery may be needed to remove part of the intestine.
In cases where the colon is enlarged, a treatment called decompression may provide relief. Decompression can be done with colonoscopy, a procedure in which a thin tube is inserted into your anus and guided into the colon. Decompression can also be done through surgery.
drug class: opioid receptor antagonist
use: constipation due to opioid use but contraindicated in suspected GI obstruction
Mnemonics: Naloxegol the naloxone that makes you go go go. Use for constipation in non-cancer pts (go go go). Naloxone - antagonist of opioid.
My conjecture for why Naloxegol is contraindicated in GI obstruction because of its abilities to make the intestine work so hard that more fecal matters from the upper parts of the GI obstructed region get moved to the GI obstructed region. This makes the matter worse -> causing GI perforation (this is my hypothesis, i couldn't look up in anywhere for the reason why)
Mnemonics for contraindications: Naloxegol the naloxone that makes you go go go that shouldn't be used when your tunnel is so obstructed as more cars are gonna be moved towards the jammed tunnel causing the perforation of the tunnel!
MOA: https://www.movantikhcp.com/about-movantik/mechanism-of-action.html
use: constipation due to opioid use but contraindicated in suspected GI obstruction
Mnemonics: Naloxegol the naloxone that makes you go go go. Use for constipation in non-cancer pts (go go go). Naloxone - antagonist of opioid.
My conjecture for why Naloxegol is contraindicated in GI obstruction because of its abilities to make the intestine work so hard that more fecal matters from the upper parts of the GI obstructed region get moved to the GI obstructed region. This makes the matter worse -> causing GI perforation (this is my hypothesis, i couldn't look up in anywhere for the reason why)
Mnemonics for contraindications: Naloxegol the naloxone that makes you go go go that shouldn't be used when your tunnel is so obstructed as more cars are gonna be moved towards the jammed tunnel causing the perforation of the tunnel!
MOA: https://www.movantikhcp.com/about-movantik/mechanism-of-action.html
Drug class: opioid antagonists
Use: hospice care in pts with advanced illness having constipation due to use of opioids
Wonder me's mnemonics: Methylnaltrexone the meth-is-now-t-rex-owns. Meth = opioids t-rex-own = opioid antagonist => constipation relieved. T-rex => very old character => hospice advanced illness
Wonder me's mnemonics for SQ only: Methylnaltrexone the meth is now-T-rex-owns. T-rex can easily lift the meth dealer just by lifting his shirt (subQ)
Use: hospice care in pts with advanced illness having constipation due to use of opioids
Wonder me's mnemonics: Methylnaltrexone the meth-is-now-t-rex-owns. Meth = opioids t-rex-own = opioid antagonist => constipation relieved. T-rex => very old character => hospice advanced illness
Wonder me's mnemonics for SQ only: Methylnaltrexone the meth is now-T-rex-owns. T-rex can easily lift the meth dealer just by lifting his shirt (subQ)
Alvimopan is indicated in people to avoid postoperative ileus following partial large or small bowel resection with primary anastomosis. Alvimopan accelerates the gastrointestinal recovery period as defined by time to first bowel movement or flatus. Alvimopan is only approved for short term use of no more than 15 doses. It is available on an inpatient basis at institutions approved by and registered with the Entereg Access Support and Education (E.A.S.E.) program. A person should receive no more than 15 doses Source: https://en.wikipedia.org/wiki/Alvimopan
Drug class: Opioid receptors antagonists
Use: accelerates GI recovery period by preventing post-op ileus following small/large bowel resection. Tho, it has serious side effects such as MI - therefore must be in REMS.
Mnemonics: Alvimopan - Alvin the chipmonk bans opioid pan pan pan! Because it ferociously bangs opioid it could cause mI in those who sees it!!! Be careful when you see Alvimopan!
Mnemonics for Alvimopan REMS: Alvimopan causes pan pan pan in the heart MI => you'll only use it in REMS sleep stages most of the time (hospitalized)
Mnemoncis for Alvimopan contraindication in liver ESRD disease: Alvimopan is banned in gan
Drug class: Opioid receptors antagonists
Use: accelerates GI recovery period by preventing post-op ileus following small/large bowel resection. Tho, it has serious side effects such as MI - therefore must be in REMS.
Mnemonics: Alvimopan - Alvin the chipmonk bans opioid pan pan pan! Because it ferociously bangs opioid it could cause mI in those who sees it!!! Be careful when you see Alvimopan!
Mnemonics for Alvimopan REMS: Alvimopan causes pan pan pan in the heart MI => you'll only use it in REMS sleep stages most of the time (hospitalized)
Mnemoncis for Alvimopan contraindication in liver ESRD disease: Alvimopan is banned in gan


Ileum: The ileum /ˈɪliəm/ is the final section of the small intestine. The ileum is the third and final part of the small intestine. It follows the jejunum and ends at the ileocecal junction, where the terminal ileum communicates with the cecum of the large intestine through the ileocecal valve.
There is no line of demarcation between the jejunum and the ileum. There are, however, subtle differences between the two:[4]
There is no line of demarcation between the jejunum and the ileum. There are, however, subtle differences between the two:[4]
- The ileum has more fat inside the mesentery than the jejunum
- The diameter of its lumen is smaller and has thinner walls than the jejunum
- Its circular folds are smaller and absent in the terminal part of the ileum
https://en.wikipedia.org/wiki/Ileum
Drug class: stool surfactant (softeners)
Wonder Me's mnemonics for Mineral oil: Mineral oil the mine era oil
Caution: binds to fat soluble ADEK vitamins => fat is the disease of the era (mineral oil) => in this era (mineral oil) it binds to all fat soluble vitamins => ADEK
Wonder Me's mnemonics for Mineral oil: Mineral oil the mine era oil
Caution: binds to fat soluble ADEK vitamins => fat is the disease of the era (mineral oil) => in this era (mineral oil) it binds to all fat soluble vitamins => ADEK
Drug class: Stool Surfactants
Wonder me's mnemonics: Glycerin the greasy soap => soap good for prevention of jammed cars but when jammed cars (constipation) already happens, soap is too little to induce release of constipation (not used for treatment of constipation).
Wonder me's mnemonics: Glycerin the greasy soap => soap good for prevention of jammed cars but when jammed cars (constipation) already happens, soap is too little to induce release of constipation (not used for treatment of constipation).
Drug class: Stool surfactant (stool softener)
Use: only used for prevention of constipation, not for treatment of constipation
MOA: Emollient laxatives, also known as stool softeners, are anionic surfactants that enable additional water and fats to be incorporated in the stool, making it easier for them to move through the gastrointestinal tract.
Use: only used for prevention of constipation, not for treatment of constipation
MOA: Emollient laxatives, also known as stool softeners, are anionic surfactants that enable additional water and fats to be incorporated in the stool, making it easier for them to move through the gastrointestinal tract.
Properties
- Site of action: small and large intestines
- Onset of action: 12–72 hours
- Examples: docusate (Colace, Diocto), Gibs-Eze[3]
Emollient agents should be taken with plenty of water. Emollient agents prevent constipation rather than treat long-term constipation.[3]
Wonder me's mnemonics for docusate : Docusate the doc-u-soap soaping your stool make it smooth with water on it. Doc-u-soap is only good for prevention because it's better to have a little soap here and there to move the cars that's not jammed when it's all jammed cars (constipation), doc-u-soap is not enough oil!
~Wonder me
Drug class: stimulant laxative
MOA: selectively directly stimulates the enteric nervous system
Mnemonics: bisa-codyl the basic(bisac) codeine (codyl) sack (-sac-)! => adjunct to codeine (opioid nervous stimulant) to sack shit!
MOA: selectively directly stimulates the enteric nervous system
Mnemonics: bisa-codyl the basic(bisac) codeine (codyl) sack (-sac-)! => adjunct to codeine (opioid nervous stimulant) to sack shit!
Senna
Ppt drug class: Stimulant Laxative
text MOA: selective action on the nerve plexus of the intestinal smooth muscle leading to enhanced motility.
Onset: rapidly => acute constipation.
Use (ppt): long-term for neurologically impaired pts & pts on opioid (together with decussate)
Wonder Me's mnemonics: Senna the sensation => sensation = nervous system => stimulant
Ppt drug class: Stimulant Laxative
text MOA: selective action on the nerve plexus of the intestinal smooth muscle leading to enhanced motility.
Onset: rapidly => acute constipation.
Use (ppt): long-term for neurologically impaired pts & pts on opioid (together with decussate)
Wonder Me's mnemonics: Senna the sensation => sensation = nervous system => stimulant
Drug class: Osmotic laxative
Wonder Me's mnemonics: Magnesium hydroxide/Magnesium Citrate the water Magnetic => osmotic!
Caution: Do NOT use for too long in renal insufficiency pts (Mg = electrolyte = renal insufficiency caution!!!!)
MOA: . The diarrhea caused by magnesium hydroxide carries away much of the body's supply of potassium, and failure to take extra potassium may lead to muscle cramps.
Magnesium citrate works by attracting water through the tissues by a process known as osmosis. Once in the intestine, it can attract enough water into the intestine to induce defecation. The additional water stimulates bowel motility. This means it can also be used to treat rectal and colon problems. Magnesium citrate functions best on an empty stomach, and should always be followed with a full (eight ounce or 25 cl) glass of water or juice to help the magnesium citrate absorb properly and help prevent any complications. Magnesium citrate solutions generally produce bowel movement in one half to six hours.
Wonder Me's mnemonics: Magnesium hydroxide/Magnesium Citrate the water Magnetic => osmotic!
Caution: Do NOT use for too long in renal insufficiency pts (Mg = electrolyte = renal insufficiency caution!!!!)
MOA: . The diarrhea caused by magnesium hydroxide carries away much of the body's supply of potassium, and failure to take extra potassium may lead to muscle cramps.
Magnesium citrate works by attracting water through the tissues by a process known as osmosis. Once in the intestine, it can attract enough water into the intestine to induce defecation. The additional water stimulates bowel motility. This means it can also be used to treat rectal and colon problems. Magnesium citrate functions best on an empty stomach, and should always be followed with a full (eight ounce or 25 cl) glass of water or juice to help the magnesium citrate absorb properly and help prevent any complications. Magnesium citrate solutions generally produce bowel movement in one half to six hours.
Ppt drug class: osmotic laxatives
MOA: PEG works to soften the fecal mass by osmotically drawing water into the GI tract. It is generally well tolerated; however, possible side effects are bloating, nausea, gas, and diarrhea (with excessive use).
Place in therapy (text): useful for acute complete bowel evacuation prior to GI examination.
Wonder Me's mnemonics: PolyEthylene Glycol the Poly water Gliding => osmotic laxative used in GI exam (think gliding the anoscope!)
MOA: PEG works to soften the fecal mass by osmotically drawing water into the GI tract. It is generally well tolerated; however, possible side effects are bloating, nausea, gas, and diarrhea (with excessive use).
Place in therapy (text): useful for acute complete bowel evacuation prior to GI examination.
Wonder Me's mnemonics: PolyEthylene Glycol the Poly water Gliding => osmotic laxative used in GI exam (think gliding the anoscope!)
Ppt indication: prophylaxis & treatment of chronic constipation
Ppt drug class: osmotic laxative
Wonder Me's mnemonics: Lactulose the lactating one => osmotic agent. Lactulose lactating causes so much fluid that it floods the tunnel causing the impacted cars (constipation) to move.
MOA (source: https://en.wikipedia.org/wiki/Lactulose): It is a disaccharide (double-sugar) formed from one molecule each of the simple sugars (monosaccharides) fructose and galactose. Lactulose is not absorbed in the small intestine nor broken down by human enzymes, thus stays in the digestive bolus through most of its course, causing retention of water through osmosis leading to softer, easier to pass stool. It has a secondary laxative effect in the colon, where it is fermented by the gut flora, producing metaboliteswhich have osmotic powers and peristalsis-stimulating effects (such as acetate), but also methane associated with flatulence. Lactulose is metabolized in the colon by bacterial flora to short chain fatty acids including lactic acid and acetic acid. These partially dissociate, acidifying the colonic contents (increasing the H+ concentration in the gut).[14]
Ppt drug class: osmotic laxative
Wonder Me's mnemonics: Lactulose the lactating one => osmotic agent. Lactulose lactating causes so much fluid that it floods the tunnel causing the impacted cars (constipation) to move.
MOA (source: https://en.wikipedia.org/wiki/Lactulose): It is a disaccharide (double-sugar) formed from one molecule each of the simple sugars (monosaccharides) fructose and galactose. Lactulose is not absorbed in the small intestine nor broken down by human enzymes, thus stays in the digestive bolus through most of its course, causing retention of water through osmosis leading to softer, easier to pass stool. It has a secondary laxative effect in the colon, where it is fermented by the gut flora, producing metaboliteswhich have osmotic powers and peristalsis-stimulating effects (such as acetate), but also methane associated with flatulence. Lactulose is metabolized in the colon by bacterial flora to short chain fatty acids including lactic acid and acetic acid. These partially dissociate, acidifying the colonic contents (increasing the H+ concentration in the gut).[14]
PPT Indication: prophylaxis & treatment for chronic constipation
Text: Glucose levels should be monitored in diabetic pts who ingest oral sorbitol
(Wonder Me's explanation: Sorbitol is a form of sugar alcohol that does not cause much increase in blood sugar as sucrose, regular sugar does but still causes an increase in blood sugar.)
Medscape dosage: 0.5-2 mL/kg up to 50 mL of 70% solution PO qDay/QID
Mnemonics: Sorbitol the sobbing one!
Sorbitol sobbing so much while sitting in the jammed car (constipation) that her crying makes a flood moving the car. Sorbitol the sobbing one. Of course, if she cries (oral one), it takes a long time to really accumulate enough to produce relief of jammed cars (constipation). However, if a lot of her coming in from the end of the tunnel (anus - enema), it's a lot! Quick relief!
Medscape:
Text: Glucose levels should be monitored in diabetic pts who ingest oral sorbitol
(Wonder Me's explanation: Sorbitol is a form of sugar alcohol that does not cause much increase in blood sugar as sucrose, regular sugar does but still causes an increase in blood sugar.)
Medscape dosage: 0.5-2 mL/kg up to 50 mL of 70% solution PO qDay/QID
120 mL of 25-30% solution PR qDay
Mnemonics: Sorbitol the sobbing one!
Sorbitol sobbing so much while sitting in the jammed car (constipation) that her crying makes a flood moving the car. Sorbitol the sobbing one. Of course, if she cries (oral one), it takes a long time to really accumulate enough to produce relief of jammed cars (constipation). However, if a lot of her coming in from the end of the tunnel (anus - enema), it's a lot! Quick relief!
Medscape:
Bioavailability: poor absorption (oral and rectal)
Metabolism: mainly in the liver to fructose
Mechanism of Action: Polyalcoholic sugar with hyper osmotic effects
http://reference.medscape.com/drug/sorbitol-342033#10
Wiki:
Sorbitol is found in some dried fruits and may contribute to the laxative effects of prunes.
Sorbitol can be used as a non-stimulant laxative via an oral suspension or enema. As with other sugar alcohols, gastrointestinal distress may result when food products that contain sorbitol are consumed. Sorbitol exerts its laxative effect by drawing water into the large intestine, thereby stimulating bowel movements.
https://en.wikipedia.org/wiki/Sorbitol
take these bulk-forming meds for the first few days
If doesn't work , take MOM if 2 days past without a bowel movement and repeat 8 hrs if have not had a bowel movement
If 3 days past, take Dulcolax
If doesn't work , take MOM if 2 days past without a bowel movement and repeat 8 hrs if have not had a bowel movement
If 3 days past, take Dulcolax
Lactulose
Sorbitol (oral route)
Indication: for chronic constipation
Lactulose only available as an oral solution
Sorbitol as an oral solution takes 1-3 days to work out
Sorbitol (oral route)
Indication: for chronic constipation
Lactulose only available as an oral solution
Sorbitol as an oral solution takes 1-3 days to work out

Source: http://www.duhs.edu.pk/curriculum/downloads/lec14-sem6-GITWK5-20140619.pdf
Psyllium < Polycarbophil < Methylcellulose
natural < semi-synthetic < synthetic
Methyl cellulose does not cause much flatulence as other products. Think: all synthetic => less side effects.
MOA (Mechanism of Action): These agents swell & distend the colons. Meaning, these agents are substances that are very gelatinous (colloids) that absorb water. Therefore, you'll need to drink water when taking these agents. These agents absorb water and cause a softening of stool mass. In addition, the bulk-forming laxatives cause an enlargement of the stools that stimulates propulsive movements in the GI tract and encourages the passage of intestinal contents (1).
Analogy: think of these bulk-forming agents like the agar powder you use to make agar gel (jello!). What do you need? water! If you just take those powder without water. What does it do? These powder may just stick to your esophagus or GI without water. Thus, you'll need water to have those agents bulk up like a real gel.
Place in therapy: maintenance therapy (in digestible)
Mnemonics:
cellulose => indigestible => laxative
Psy sings Polly's got a car she loves must've met the sell-or-lose criteria working hard to bulk up his belly. He looks constipated!
Psy: psy singer => Psyllium
Polly's got a car she loves: Polycarbophil
Met the sell or lose: Methylcellulose
Bulk: bulking agents

(1): http://pharmacy.utah.edu/pharmtox/common_meds/icm15.html
(2): https://books.google.com/books?id=XT3eAAAAQBAJ&pg=PA67&lpg=PA67&dq=Psyllium++Polycarbophil++Methylcellulose+mnemonics&source=bl&ots=UcfnsRHYp9&sig=Wz46D_hXvMRfGDKtfiwCgU2HImU&hl=en&sa=X&ved=0ahUKEwjAnNTX9sbMAhUK4mMKHcofBjoQ6AEIHDAA#v=onepage&q=Psyllium%20%20Polycarbophil%20%20Methylcellulose%20mnemonics&f=false
natural < semi-synthetic < synthetic
Methyl cellulose does not cause much flatulence as other products. Think: all synthetic => less side effects.
MOA (Mechanism of Action): These agents swell & distend the colons. Meaning, these agents are substances that are very gelatinous (colloids) that absorb water. Therefore, you'll need to drink water when taking these agents. These agents absorb water and cause a softening of stool mass. In addition, the bulk-forming laxatives cause an enlargement of the stools that stimulates propulsive movements in the GI tract and encourages the passage of intestinal contents (1).
Analogy: think of these bulk-forming agents like the agar powder you use to make agar gel (jello!). What do you need? water! If you just take those powder without water. What does it do? These powder may just stick to your esophagus or GI without water. Thus, you'll need water to have those agents bulk up like a real gel.
Place in therapy: maintenance therapy (in digestible)
Mnemonics:
cellulose => indigestible => laxative
Psy sings Polly's got a car she loves must've met the sell-or-lose criteria working hard to bulk up his belly. He looks constipated!
Psy: psy singer => Psyllium
Polly's got a car she loves: Polycarbophil
Met the sell or lose: Methylcellulose
Bulk: bulking agents
 |
| Psy sings Polly's got a car she loves must've met the sell-or-lose criteria. He's working hard to bulk up his belly. He looks constipated! |

(1): http://pharmacy.utah.edu/pharmtox/common_meds/icm15.html
(2): https://books.google.com/books?id=XT3eAAAAQBAJ&pg=PA67&lpg=PA67&dq=Psyllium++Polycarbophil++Methylcellulose+mnemonics&source=bl&ots=UcfnsRHYp9&sig=Wz46D_hXvMRfGDKtfiwCgU2HImU&hl=en&sa=X&ved=0ahUKEwjAnNTX9sbMAhUK4mMKHcofBjoQ6AEIHDAA#v=onepage&q=Psyllium%20%20Polycarbophil%20%20Methylcellulose%20mnemonics&f=false
Source: https://np.reddit.com/r/explainlikeimfive/comments/2zyf5a/eli5_why_does_diarrhea_come_so_quickly_when_food/cpnq0wx?context=3
So your bowels are like a long train track and your food is like a set of cars on the track. Transit time between Point A, your mouth, and Point B, the chute, is a bit flexible but normally operates on a regularly scheduled basis.
When you eat, you put cars on the track and send them to Point B. As these cars go to Point B, they lose passengers (nutrients) at various points in the thin tunnel portion (small intestine). The journey isnt complete and the journey has already altered the shape of the car pretty significantly giving a rusty color. Once in the larger portion of the tunnel, the cars are checked for stray passengers and are hosed down a bit so that transition out of Point B isn't so bad. Sometimes, the train cars park juuust outside the gates of Point B so they can exit at the best time for the operator (toilet).
Wonder Me's constipation analogy: Constipation occurs when either the stool itself is too hard, i.e., the cars have no oil to really work. Therefore, you'll need agent to work on the stool. Or, it could be because of the track (the intestinal wall itself) that's malfunctioning. So, you'll need agents to work on the track too.
vedolizumab
natalizumab
infliximab
adalimumab
certolizumab
Mnemonics: Vedette Natalie inflicted an AyayaDA certificate on those with IBD. (Remember Natalie had diarrhea? Remember she brought in all of those new ADA - American Diabetes Association carb count list?)
Vedette => vedolizumab
Natalie => natalizumab
Inflicted => infliximab
AyayaDA => adalimumab
certificate => certolizumab
mab => injections only (remember my bf says: noo my allergies are not that bad to be on Omalizumba. Isn't that one an injection? Also it's so expensive!!!!)
Natalizumab => REMS for PML.
Mnemonics: Natalie's getting older with white hair in different spots on her head (PML: Progressive Multifocal Leukoencephalopathy)
Certolizumab/Natalizumab => for Crohn's disease only.
Mnemonics: C for C as Certolizumab for Crohn's Natalie likes to inflict so it's she always has to go with C.
PPD prior to therapy to r/o TB? => Remember how Natalie always is very strict on TB? Need to administer PPD prior to therapy (prior to registration!)
~Wonder Me~
natalizumab
infliximab
adalimumab
certolizumab
Mnemonics: Vedette Natalie inflicted an AyayaDA certificate on those with IBD. (Remember Natalie had diarrhea? Remember she brought in all of those new ADA - American Diabetes Association carb count list?)
Vedette => vedolizumab
Natalie => natalizumab
Inflicted => infliximab
AyayaDA => adalimumab
certificate => certolizumab
mab => injections only (remember my bf says: noo my allergies are not that bad to be on Omalizumba. Isn't that one an injection? Also it's so expensive!!!!)
Natalizumab => REMS for PML.
Mnemonics: Natalie's getting older with white hair in different spots on her head (PML: Progressive Multifocal Leukoencephalopathy)
Certolizumab/Natalizumab => for Crohn's disease only.
Mnemonics: C for C as Certolizumab for Crohn's Natalie likes to inflict so it's she always has to go with C.
PPD prior to therapy to r/o TB? => Remember how Natalie always is very strict on TB? Need to administer PPD prior to therapy (prior to registration!)
~Wonder Me~
TNF caused inflammation in the intestines.
http://www.hindawi.com/journals/mi/2014/325129/
Anti-tumor necrosis factor (anti-TNF) drugs are a class of drugs that are used worldwide to treat inflammatory conditions. These drugs are able to reduce inflammation and stop disease progression. TNF is a chemical produced by the immune system that causes inflammation in the body. In healthy individuals, excess TNF in the blood is blocked naturally, but in those who have rheumatic conditions, higher levels of TNF in the blood lead to more inflammation and persistent symptoms. - See more at: http://www.rheumatology.org/I-Am-A/Patient-Caregiver/Treatments/Anti-TNF#sthash.lHeh5Bk1.dpuf -
The primary role of TNF is in the regulation of immune cells. TNF, being an endogenous pyrogen, is able to induce fever, apoptotic cell death, cachexia, inflammation and to inhibit tumorigenesis and viral replication and respond to sepsis via IL1 & IL6 producing cells. Dysregulation of TNF production has been implicated in a variety of human diseases including Alzheimer's disease,[2] cancer,[3] major depression,[4] Psoriasis[5] and inflammatory bowel disease (IBD).[6] While still controversial, studies of depression and IBD are currently being linked to TNF levels.[7]
Impaired cell death program has been noted as one of the hallmarks of chronic lymphocytic leukemia (CLL) and contributes to its accumulation of malignant monoclonal B cells as well as to chemotherapy resistance. A cell can die through the apoptosis or necrosis pathway. Recent investigations suggest that in apoptotic-deficient conditions, such as most types of cancer, a process of programmed necrosis, called necroptosis, prevails. source: http://www.nature.com/leu/journal/v26/n6/full/leu2011357a.html
http://www.hindawi.com/journals/mi/2014/325129/
Anti-tumor necrosis factor (anti-TNF) drugs are a class of drugs that are used worldwide to treat inflammatory conditions. These drugs are able to reduce inflammation and stop disease progression. TNF is a chemical produced by the immune system that causes inflammation in the body. In healthy individuals, excess TNF in the blood is blocked naturally, but in those who have rheumatic conditions, higher levels of TNF in the blood lead to more inflammation and persistent symptoms. - See more at: http://www.rheumatology.org/I-Am-A/Patient-Caregiver/Treatments/Anti-TNF#sthash.lHeh5Bk1.dpuf -
The primary role of TNF is in the regulation of immune cells. TNF, being an endogenous pyrogen, is able to induce fever, apoptotic cell death, cachexia, inflammation and to inhibit tumorigenesis and viral replication and respond to sepsis via IL1 & IL6 producing cells. Dysregulation of TNF production has been implicated in a variety of human diseases including Alzheimer's disease,[2] cancer,[3] major depression,[4] Psoriasis[5] and inflammatory bowel disease (IBD).[6] While still controversial, studies of depression and IBD are currently being linked to TNF levels.[7]
Impaired cell death program has been noted as one of the hallmarks of chronic lymphocytic leukemia (CLL) and contributes to its accumulation of malignant monoclonal B cells as well as to chemotherapy resistance. A cell can die through the apoptosis or necrosis pathway. Recent investigations suggest that in apoptotic-deficient conditions, such as most types of cancer, a process of programmed necrosis, called necroptosis, prevails. source: http://www.nature.com/leu/journal/v26/n6/full/leu2011357a.html
2 types of corticosteroids.
Corticosteroids are a class of steroid hormones that are produced in the adrenal cortex of vertebrates, as well as the synthetic analogues of these hormones. Corticosteroids are involved in a wide range of physiological processes, including stress response, immune response, and regulation of inflammation, carbohydrate metabolism, protein catabolism, blood electrolyte levels, and behavior.
- Glucocorticoids such as cortisol control carbohydrate, fat and protein metabolism, and are anti-inflammatory by preventing phospholipid release, decreasing eosinophil action and a number of other mechanisms.[2]
- Mineralocorticoids such as aldosterone control electrolyte and water levels, mainly by promoting sodium retention in the kidney.
Glucocorticoids (GCs) are a class of corticosteroids, which are a class of steroid hormones. Glucocorticoids are corticosteroids that bind to the glucocorticoid receptor (GR),[1] that is present in almost every vertebrate animal cell. The name glucocorticoid (glucose + cortex + steroid) is composed from its role in regulation of glucose metabolism, synthesis in the adrenal cortex, and its steroidal structure (see structure to the right). A less common synonym is glucocorticosteroid.
GCs are part of the feedback mechanism in the immune system which reduces certain aspects of immune function, such as reduction of inflammation. They are therefore used in medicine to treat diseases caused by an overactive immune system, such as allergies, asthma, autoimmune diseases, and sepsis. GCs have many diverse (pleiotropic) effects, including potentially harmful side effects, and as a result are rarely sold over the counter.[2] They also interfere with some of the abnormal mechanisms in cancer cells, so they are used in high doses to treat cancer. This includes: inhibitory effects on lymphocyte proliferation as in the treatment of lymphomas and leukemias; and the mitigation of side effects of anticancer drugs.
Source: https://en.wikipedia.org/wiki/Glucocorticoid

